what percentage of total shoulder complex motion is attributed to the glenohumeral joint
Original Editor - Venus Pagare
Meridian Contributors - Mathieu Vanderroost, Venus Pagare, Nikhil Benhur Abburi, Chelsea Mclene, Kim Jackson, Vidya Acharya, Admin, Kai A. Sigel, WikiSysop, Claire Knott, Wanda van Niekerk, Rachael Lowe and Naomi O'Reilly
Introduction [edit | edit source]
Scapulohumeral rhythm (also referred to as glenohumeral rhythm) is the kinematic interaction between the scapula and the humerus, first published by Codman in the 1930s. [ane]
This interaction is of import for the optimal function of the shoulder. [2] When in that location is a alter of the normal position of the scapula in relation to the humerus, this can cause a dysfunction of the scapulohumeral rhythm. The alter of the normal position is also called scapular dyskinesia. Diverse studies of the machinery of the shoulder articulation have attempted to describe the global movement chapters of the shoulder refer to that description, can you evaluate the shoulder to run across if the function is correct? and explain the complex interactions between components involved in placing the hand in space.[3]
Clinical Relevant Beefcake [edit | edit source]
Shoulder Movements [edit | edit source]
The interplay of 4 articulations (Sternoclavicular Joint, Acromioclavicular Articulation, Scapulothoracic Joint and Glenohumeral Articulation) of the shoulder complex, results in a coordinated motion design of the arm elevation. The involved movements at each joint are continuous, although occurring at various rates and at different phases of arm elevation. The movement of the scapula can be described by rotations in relation to the thorax. The scapula moves around a dorso-ventral axis, resulting in a rotation in the frontal plane. In this movement the glenoid cavity is turned cranially (upwards rotation) or caudally (downward rotation). In the sagittal plane, around a latero-lateral axis the scapula rotates posteriorly (posterior tilting) or anteriorly (inductive tilting). External and internal rotation occurs effectually a cephalo-caudal (longitudinal) axis. The external rotation brings the glenoid cavity more than into the frontal plane, whereas the internal rotation turns the glenoid cavity more than to the sagittal airplane. [4]
When nosotros perform flexion, the glenohumeral (GH) joint contributes 100°-120°. The scapula on the thorax contributes to peak (flexion and abduction) of the humerus by upwardly rotating the glenoid fossa 50° to 60° from its resting position.[1] If the humerus were fixed to the fossa, this lonely would result in up to 60° of pinnacle of the humerus. The humerus, of form, is not stock-still merely can motility independently on the glenoid fossa.
Inman et al. reported an inconsistent amount and type of scapular motion in relation to GH-motion during the initial sixty°. [v] In this early on phase (0-threescore°), motion occurs primarily at the GH joint, although stressing the arm may increase the scapular contribution. [6] During abduction of the humerus in the plane of the scapula, an boilerplate of 43° of lateral rotation from the resting position has been reported, with peak lateral rotation mostly occurring between 90° and 120° of humeral acme. Information technology must as well be recognized, however, that elevation of the arm is often accompanied non only past height of the humerus but also by lateral rotation of the humerus in relation to the scapula. [7]
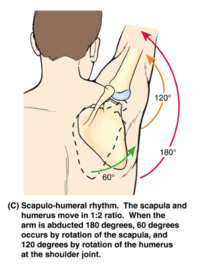
When we perform abduction, the GH-joint contributes xc-120°. The combination of scapular and humeral move result in a maximum range of height of 150-180°. [8] [9] Also by abduction Inman et al. reported an inconsistent amount and type of scapular motion in relation to GH-movement this time during the initial 30°. [five] In this early phase, movement occurs primarily at the GH articulation, although stressing the arm may increase the scapular contribution. [6]
Scapulohumeral Rhythm [edit | edit source]
It describes timing of movement at glenohumeral and scapulothoracic joint during shoulder elevation.
Get-go 30 degrees of shoulder elevation involves a "setting stage":
- The movement is largely glenohumeral.
- Scapulothoracic move is small and inconsistent.
And later the offset 30 degrees of shoulder elevation:
- The glenohumeral and scapulothoracic joints move simultaneously.
- Overall ii:1 ratio of glenohumeral to scapulothoracic move.
Scapulohumeral rhythm tin can be observed by palpating the scapula's position as a person elevates the shoulder. Scapular landmarks for palpation are the base of the spine and the junior angle.
Scapulohumeral rhythm serves two purposes:
- Information technology preserves the length-tension relationships of the glenohumeral muscles. Muscles exercise not shorten as much as they would without the scapula's upward rotation, and and then can sustain their force production through a larger portion of the range of movement.
- It prevents impingement betwixt the humerus and the acromion. Subacromial impingement can occur unless relative move between the humerus and scapula is limited because of the difference in size between the glenoid fossa and the humeral caput. Simultaneous movement of the humerus and scapula during shoulder summit limits relative (arthrokinematic) movement between the ii bones.[x] [11] [12]
Scapulohumeral Ratio [edit | edit source]
Scapulohumeral rhythm or ratio is significantly greater (less scapular motion and more than humeral motility) in the sagittal plane than other planes. Consistent with the findings, the dominant side demonstrated significantly higher values for SH rhythm than the non-dominant side but only in the coronal and scapular planes but not in the sagittal plane. [9] By healthy male is a pregnant difference by hand dominance only in scapular upwardly rotation during scapular aeroplane arm elevation.[7]
The scapulohumeral rhythm is therefore defined as the ratio of the glenohumeral movement to the scapulothoracic motion during arm pinnacle. This is most often calculated by dividing the total amount of shoulder elevation (humerothoracic) by the scapular upward rotation (scapulothoracic). [four]
In the literature Scapulohumeral rhythm is described like a ratio: humeral pinnacle : scapulothoracal rotation. The overall ratio of 2:1 during arm acme is commonly used. According to the 2-to-1 ratio frame-work, flexion or abduction of ninety° in relation to the thorax would exist achieved through approximately lx° of GH and 30° of ST motion. In another study of Scapulohumeral rhythm betwixt children and adults, the mean ratio for the scapular airplane was 2.4:ane for adults, 1.three:1 for children. [5]
If we compare the scapulohumeral rhythm by children with adults, we run into that children showed a higher scapulohumeral rhythm during lowering of the arm than adults. [1] Besides during scapular plane rotation from 25° to 125°, children showed greater upwardly rotation than adults. [5]
Ratios are often described every bit nonlinear indicating changing ratios during ROM. The ii to one ratio essentially varies in scapular and humeral contributions at different points in the ROM and among individuals.
[thirteen]
Epidemiology / Etiology [edit | edit source]
It has been reported that scapular dyskinesis occurs in 68 - 100% of patients with shoulder injuries (including glenohumeral instability, rotator cuff abnormalities, and labral tears. [8] Other studies showed that scapular upward rotation is significantly increased in patients with full-thickness rotator gage tears compared with controls in both sagittal and scapular plane elevation. Besides, an increased scapular component is generally thought to contribute to the scapulohumeral rhythm ratio in frozen or stiff shoulders. [9]
Given the office of the scapula in shoulder function, the power to monitor the coordinated motion of the scapula and humerus (scapulohumeral rhythm) may accept clinical implications when dealing with overhead athletes and patients with shoulder pathologies.[1]
Sports participation results in slight differences in side-to-side motility and in scapular resting position in overhead athletes. [5] [4] Overhead athletes have some disproportion in scapular upward rotation and scapulohumeral rhythm ratio between dominant and non-dominant shoulder. It should non exist considered automatically as a pathological sign merely rather an adaptation to sports practice and extensive use of upper limb. [9]
People with college BMI have scapula kinematic patterns different from people with lower BMI. They have increased scapula upward rotation during arm elevation. [six]
Characteristics / Clinical Presentation [edit | edit source]
Scapulohumeral rhythm is a common metric for assessing musculus function and shoulder articulation motion.[7] There is a three-dimensional scapular kinematic pattern during normal arm elevation that include upward rotation, posterior tilting and varying internal/external rotation dependent on the airplane and angle of peak. [one] [2] When at that place is change of the normal position of the scapula related to the humerus, the scapulohumeral rhythm is disturbed.
Differential Diagnosis [edit | edit source]
There isn't really a differential diagnosis for scapulohumeral rhythm disorders. But there are multiple causes for scapular dyskinesia and scapulohumeral rhythm disorders. [4] Causative factors can exist grouped into:
- Bony causes include thoracic kyphosis or clavicula fracture.
- Joint causes include high grade Air conditioning instability, Air-conditioning arthrosis and instability, and GH joint internal derangement.
- Neurological causes include Cervical Radiculopathy, long thoracic or spinal accompaniment nerve palsy.
- Inflexibility causes, for example: inflexibility and stiffness of the pectoralis modest and biceps short head tin can create inductive tilt and protraction due to their pull on the coracoid. [4] Soft tissue posterior shoulder inflexibility can lead to GH internal rotation deficit (GIRD), which creates a 'wind-upwards' of the scapula on the thorax with reduced humeral internal rotation and horizontal abduction.
- Muscular causes: Serratus anterior activation and strength is decreased in patients with impingement and shoulder pain, contributing to the loss of posterior tilt and upward rotation causing dyskinesis. [8] [half-dozen] In improver, the upper trapezius/lower trapezius forcefulness couple may be contradistinct, with delayed onset of activation in the lower trapezius, which alters scapular upward rotation and posterior tilt. Altered scapular motion or position both decrease linear measures of the subacromial space [vii] [2], increase impingement symptoms, decrease rotator cuff force [14], increase strain on the anterior GH ligaments [15]
Alterations in scapular position and control afforded by the scapula stabilizing muscles are believed to disrupt stability and role of the glenohumeral articulation [2] [14] [15], thereby contributing to shoulder impingement, rotator gage pathology and shoulder instability. [1]
Diagnostic Procedures [edit | edit source]
Inman, Saunders and Abbott were the get-go to measure scapulohumeral rhythm using radiography and suggested what became the widely accepted two:1 ratio between glenohumeral elevation and scapulothoracic (ST) up rotation (SUR). [8]
Since then imaging modalities (X-ray and magnetic resonance imaging)[nine], cinematography [5], goniometry [iv] [6] [vii], and more than recently iii-dimensional tracking systems[2] [14] [15]
Outcome Measures [edit | edit source]
The Simple Shoulder Exam (SST) is an internationally used patient-reported upshot for clinical practice and enquiry purposes. It was developed for measuring functional limitations of the affected shoulder in patients with shoulder dysfunction and contains 12 questions (yes/no). It is a reliable and valid musical instrument for evaluating functional limitations in patients with shoulder complaints. [14]
Other frequently used questionnaires are: the Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire, the Shoulder Pain and Inability Index (SPADI) and the American Shoulder and Elbow Surgeons (ASES) score. These questionnaires take been shown acceptable for clinical use. [15] These questionnaires are non specific for scapulohumeral rhythm disorders, but may help in the diagnostic process.
Examination [edit | edit source]
Observation and examination of the scapulohumeral rhythm is commonly performed by physical therapists during postural and shoulder examinations. The notion of a proper "rhythm" is routinely used to describe the quality of motility at the shoulder complex.[two]
Clinical measures (inclinometer, tape measure) are only capable of measuring scapular kinematics 2-dimensionally.
The inclinometer is capable of measuring angles (in degrees) from a horizontal reference to appraise static positions of scapular upwards rotation, this upward rotation can easily exist used by clinicians when evaluating the scapular motion. Different authors take demonstrated that these clinical assessments give valid and accurate information regarding scapular kinematics. [half dozen] [7] [ii]
Linear assessment using tape measures tin be used to examine possible asymmetries and patterns of aberrant motion betwixt the pathological and good for you scapula. This examination is based on uncomplicated bilateral visual observation of scapular position. [15] Although this method is a subjective approach, inquiry gave show that it is a qualitative method. [one]
Quantitative measurement of scapular positioning tin also be achieved with LSST (lateral scapular slide test). This test evaluates the scapular symmetry while varying loads are placed on the supporting musculature. Three positions of the upper extremities are proposed:
- Position i, the bailiwick's arm is relaxed at the side (0° of humeral elevation).
- Position ii, the subject area places his or her hand on the lateral iliac crest.
- Position 3, corresponds to an internally rotated and abducted arm to 90°.
Ii measurements are performed using a record in each position (between the inferior bending of the scapula and the closest spinous process) in order to allow calculation of an average value. [half-dozen]
A one.5-cm asymmetry in any of the positions is established as a threshold for an abnormal pattern.
Intratester reliability of the Kibler LSST method ranged from good to loftier, although the intertester reliability was poor. [14] Nijs et al. observed coefficients of >0.70 (interobserver reliability in intraclass correlation coefficients). The clinical importance of the tests' outcomes, however, is questionable. [6] [15]
Another test is the SDT (scapular dyskinesis test). The SDT is a visually based test for scapular dyskinesis that involves a patient performing weighted shoulder flexion and abduction movements while scapular motion is visually observed. This test consists of characterizing scapular dyskinesis as absent or present and each side is rated separately. Dyskinesis is defined equally the presence of either winging (prominence of whatever portion of the medial edge or junior angle away from the thorax) or dysrhythmia (premature, or excessive, or stuttering motion during elevation and lowering). [ix] Good inter-rater reliability of this test (75–82% understanding; weighted κ=0.48–0.61) was achieved. [five]
Medical Management [edit | edit source]
Optimal rehabilitation of scapulohumeral rhythm disorders requires addressing all the causative factors that can create the dyskinesis and and so restoring the rest of musculus forces that allow scapular position and move. [7]
Physical Therapy Management [edit | edit source]
It is essential to make a diagnosis nigh the cause of the scapulohumeral rhythm dysfunction earlier starting physical therapy. For example 'Winged scapula' of the scapula may be acquired by a paresis of the muscle Serratus Anterior or by a dysfunction of the musculus Trapezius.
Both passive and active movement disturbances can cause a scapulohumeral rhythm dysfunction. Causes may exist: shortening of muscles like one thousand. Pectoralis Modest, chiliad. Latissimus Dorsi and one thousand. Levator Scapulae, shortening of the posterior joint capsule and/or lack of coordination between essential muscles similar the g. Serratus Anterior, m. Trapezius and Rotator cuff muscles. [2]
It may be articulate that every therapy should exist individualized.
Lengthening of muscles or connective tissue must be done by stretching and/or agile and passive mobilizations. It's of import that the patient gets a dwelling exercise program to go on stretching and mobilizations. [ane] Center thoracic manipulations in seated position have no influence on the scapulohumeral rhythm and scapular kinematics during arm flexion and thus should be avoided. [fifteen]
Training the coordination betwixt muscles should be washed in ii phases. Phase one will include the 'setting' of the muscles. In this phase the patient will learn how to subtle contract his muscles. Tactile feedback or myofeedback may exist necessary during this phase. Practicing at abode is of import to railroad train the duration of muscle contraction and train in other positions and so that contraction is possible in every posture of daily life. In phase 2 the contraction should be automated. This can be trained with stabilization exercises. Exercises on the back should be avoided because muscles should stabilize the scapula instead of the ground. The stabilization exercises should be static and dynamic. [ane] Examples of exercises are: push up plus, press-up, low-rowing, horizontal abduction, serratus punch and dynamic hug. [1]
Muscles should exist trained in functional patterns (sport or activity specific patterns) instead of isolated patterns considering it will cause maximal scapular muscle activations. [6]
Most abnormalities will occur in the eccentric phase of movements or with a lot of repetitions (fatigue). So it's of import not to forget to train the eccentric phase and endurance of the muscles. [14]
With shoulder patients you should e'er be aware of the influence on the spine. Some patients could have a loftier caste of Thoracic Hyperkyphosis which can exist treated with active and passive mobilizations of the thoracic spine. [15]
References [edit | edit source]
- ↑ 1.0 1.i 1.ii ane.3 1.4 i.5 ane.6 i.7 i.eight ane.nine Codman EA: The Shoulder,Boston: G.Miller & Company,1934
- ↑ 2.0 ii.ane ii.ii 2.three 2.iv 2.five 2.vi two.7 Kibler WB. The role of the scapula in athletic shoulder part. Am J Sports Med 1998;26:325-337
- ↑ Cathcart CW: Movements of the shoulder girdle involved in those of the arm on the body. J Anat Physiol 1884; 18:209-218.
- ↑ iv.0 iv.one 4.ii 4.3 four.four 4.5 Struyf, F., Scapular positioning and move in unimpaired shoulders, shoulder impingement syndrome, and glenohumeral instability, Scandinavian Journal of Medicine and Science in sports, jrg20, nr3, 2011, p352
- ↑ 5.0 5.i 5.ii 5.iii 5.4 5.5 5.6 Inman B, Saunders J, Abbott L: Observations of office of the shoulder joint. J Bone Articulation Surg Br 2004; 26:i.
- ↑ 6.0 half dozen.1 6.2 6.3 six.4 half-dozen.5 6.6 6.vii six.viii Lockhart RD. Movements of the Normal Shoulder Joint and of a case with Trapezius Paralysis studied by Radiogram and Experiment in the Living. J Anat 1930; 64: 288-302.
- ↑ 7.0 7.i 7.2 seven.3 7.4 7.5 7.6 McQuade K, Smidt G: Dynamic scapulohumeral rhythm: The effects of external resistance during summit of the arm in the scapular aeroplane. J Orthop Sports Phys Ther 1998; 27:125–133.
- ↑ 8.0 viii.ane 8.2 8.iii Rundquist P, Anderson DD, Guanche CA, et al. Shoulder kinematics in subjects with frozen shoulder. Arch Phys Med Rehabil 2003; 84:1473–1479.
- ↑ nine.0 9.1 9.2 9.3 nine.4 ix.5 Barnes CJ, Van Steyn SJ, Fischer RA: The effects of age, sex, and shoulder potency on range of motion of the shoulder. J Shoulder Elbow Surg 2001; x:242– 246.
- ↑ Crosbie J, Kilbreath SL, Hollmann L, York S. Scapulohumeral rhythm and associated spinal motion. Clinical biomechanics. 2008 Feb 1;23(ii):184-92.
- ↑ Sugamoto K, Harada T, Machida A, Inui H, Miyamoto T, Takeuchi Eastward, Yoshikawa H, Ochi T. Scapulohumeral rhythm: relationship betwixt movement velocity and rhythm. Clinical Orthopaedics and Related Inquiry (1976-2007). 2002 Aug i;401:119-24.
- ↑ scapulo humeraal rhythm. acedemy of clinical massage. Available from https://www.academyofclinicalmassage.com/the-scapulohumeral-rhythm/ [last accessed 11/01/2021]
- ↑ Educom Standing Education Scapulohumeral Rhythm - A Chiropractic Online CE™Production Available from https://www.youtube.com/lookout man?v=H4nfQEeJmFo&characteristic=emb_logo
- ↑ 14.0 14.1 14.2 14.3 xiv.4 14.five Smith J et al., Effect of scapular protraction and retraction on isometric shoulder superlative strength. Arch Phys Med Rehabil 2002;83:367–seventy.
- ↑ xv.0 fifteen.1 xv.2 15.3 15.4 fifteen.5 xv.vi xv.seven Cleland J: A lecture on the shoulder girdle and its movements. Lancet 1881;i:11-12.
Source: https://www.physio-pedia.com/Scapulohumeral_Rhythm
0 Response to "what percentage of total shoulder complex motion is attributed to the glenohumeral joint"
Post a Comment